Heroic Failures in Sample Preparation


We were recently flattered to participate in ChromTalks, a virtual symposium put on by LCGC and CHROMacademy. Unlike conventional scientific symposia, this was touted as highly experienced speakers from industry and academia imparting key learnings from their long experience with chromatography, from heroic failures that have taught them valuable lessons, to moments of inspirational serendipity, and everything in between. This month, we present additional perspectives from our presentation. Particularly, we discuss health and safety considerations along with the role of training programs, and other often overlooked factors that may improve laboratory efficiency in the long run.
I have to admit I was a little bit flattered when asked, as an experienced chromatographer, to share the wisdom of our group’s years with a broad audience at ChromTalks. However, when I was asked to focus on our group’s failures, my emotions were crushed for a moment, until I realized they must know me too well.
For the balance of this column, I capitalize on the numerous mistakes made during the course of our career (and trust me, there have been plenty), so that you can either learn from my failures in the sample preparation realm, or laugh at my expense. Let’s discuss seven different case studies, some rather simple and somewhat humorous, and others much more serious.
Case Study #1: Flatlined
The first of these failures happened in my first job after I earned my Master’s degree, where I primarily used liquid chromatography (LC). Because it took place in a regulated laboratory, I had very little experience in maintaining a chromatographic system, and, especially back in the day, I was not a very mechanical person. Later, at my first professional meetings, I heard Colin Poole claim that in the parking lot of any chemistry facility, the old, beat-up cars likely belonged to the chromatographers because they’re the ones that know how to fix equipment.
When I began my first job, I was replacing a long-time technician, and she was more interested in the social aspects of saying goodbye to all of her friends. As a result, my initial training involved reading the instrument manuals for a Varian 3700 gas chromatograph (GC) and a Hewlett-Packard 5880 GC, the two workhorses of the laboratory. Those of you that remember a Hewlett-Packard 5880 are not only getting old, like me, but remember that you had to be a bit of a master plumber to really understand its operation.
As you can imagine, those instrument manuals were not the most exciting reading in the world to a young twenty-something embarking on a new career. I had a good half day, maybe a full day, of actual training, during which I was shown some of laboratory’s practices and developed methods. The following Monday, I was on my own. During my undergraduate and MS programs, I had heard about the safety concerns associated with gas cylinders, so I was proud of myself that Monday morning when I was able to replace the hydrogen cylinder without any problem, until I injected the my first sample and saw no peaks. There would be several feet of paper on the floor (this was in the days of the strip-chart recorder) with nothing but a flat line. I checked everything; there were no leaks, all the valves were correctly open or closed, and so forth.
Finally, over lunch, I realized that yes, the flame ionization detector requires a flame and, as observed in Figure 1, the flame requires air and some kind of fuel gas. That fuel gas is hydrogen. When the hydrogen is disconnected to replace the cylinder, the flame goes out. Once the flame was reignited, everything worked great, and I was well on my way toward what has been a somewhat successful career.

, as is used in capillary GC. Diagram courtesy of CHROMacademy.")
FIGURE 1: Schematic diagram of a flame ionization detector (FID), as is used in capillary GC. Diagram courtesy of CHROMacademy.
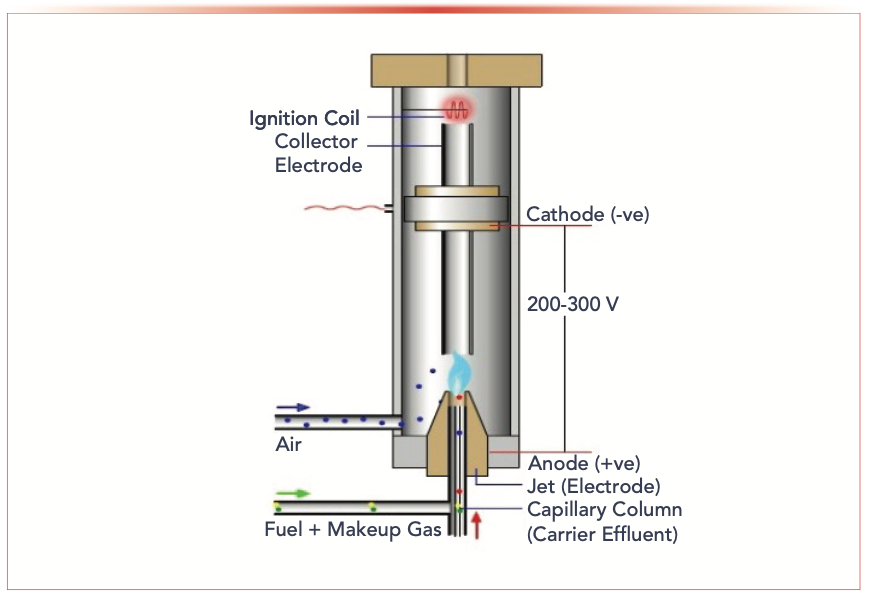
The lesson from this case study is to know your system and its operation. When I teach chromatography troubleshooting, one of the first lessons taught is that whenever you encounter a unique situation, you need to ask questions—what did you do differently, what changes were made, and so forth. Perhaps ask the questions repeatedly, in different ways, to uncover the causes of the problem you are troubleshooting. A second lesson is to evaluate your training programs for new laboratory employees.
Case Study #2: The Big Bang
The next case study occurred when I was in graduate school in Milton Lee’s group at Brigham Young University in the late 1980s, as he was developing Lee Scientific to bring capillary supercritical fluid chromatography (SFC) to the market. The company was evaluating different pumps and ovens from different vendors. Throughout the laboratory, we had a variety of SFC systems that Professor Lee and his graduate students had developed over the years. Each graduate student had a dedicated system, with unique detectors, cosolvent pumps, and injectors. Students often swapped system components depending on the needs of a project.
Because of all of the changes, including software upgrades, the system I was using had a software bug. First, you must know that these systems had a rotary valve, like an injector in an LC system, connecting the carbon dioxide supply tank, the CO2 pump, the cosolvent pump, and the chromatography system. What happened in my particular system was that after the syringe pump was refilled, the valve entered a continuous loop, cycling through all positions. Since I was aware of this, I simply exited the program each time I refilled the pump, and things would return to normal.
That is, until one evening when I went to the other end of the laboratory to talk to some of my fellow students. Before long, there was a loud explosion, not unlike a shotgun had been set off next to my ear. One of the plastic-coated glass solvent bottles had shattered. What happened was every time it connected the CO2 cylinder to that bottle, it released a little pressure into that solvent bottle, eventually causing it to explode. Luckily, no one was hurt.
The Lee Scientific folks came down the next morning and did a very thorough investigation. I found out a lot about how companies perform failure analysis of their equipment. I think the likelihood of this happening again is much more remote than back in the mid-1980s, given that there’s much more awareness of safety and training, as well as the development of the safety culture.
Once again our lesson is to know your system, but the corollary is that if something isn’t working properly, don’t just try to work around the system as I did. Don’t be afraid to ask questions, find the appropriate cause (the software, in my case), and actually fix the problem.
Case Study #3: Up in Flames
This one occurred after I started at the university and I was teaching instrumental analysis, around the time of the height of popularity of the television show “CSI.” I would end the semester with a forensics project. We would have a mock crime scene, and each student would receive one piece of evidence for analysis, with half of the students working for the prosecution and half for the defense. At the closing trial, they would provide testimony on their evidence with cross-examination by their classmates.
I would develop an elaborate crime scene; one year, that was based on a fire at a meth laboratory. Much of the evidence involved the household products (cold and cough pills, common solvents, and so forth) used in the illicit manufacture of methamphetamine. For example, at the time, you would see the kind of posters shown in Figure 2 in the back of certain retail stores. One of the items was matches used for the phosphorus. To obtain a piece of evidence and somewhat conceal it, I took the matches, cut off the head of the match, then ground it with a mortar and pestle.

FIGURE 2: Example of warning posters to retail employees to curb the availability of household products used in the illicit manufacture of methamphetamine.

All of a sudden, there was a giant flame! It should have been common sense, but if you think about what happens when you grind a “strike anywhere” match with a mortar and pestle, yes, the matches are going to ignite.
The lesson to be learned from this case study is to know your sample. The corollary is to not allow our familiarity with the sample lull us into a false sense of safety as we process our samples.
Case Study #4: Powdered Pringles
Our fourth case study is another simple, and humorous, example. While I worked at Procter & Gamble, we were looking at the fat content of Pringles brand potato crisps. I believe I was comparing different extraction procedures like pressurized liquid extraction (PLE), supercritical fluid extraction (SFE), and microwave assisted extraction (MAE).
To improve the extraction, I needed to grind the sample and mix it with diatomaceous earth. For almost all of our sample extraction methods for solids, we generally want our sample to be in the form of a free-flowing powder. In this case, I used an inexpensive coffee mill rather than a standard analytical mill. Keep in mind that this was in the mid-1990s, so coffee mills weren’t as sophisticated as the one you might have in your kitchen today. Nowadays, you can disassemble the mill to clean the blades and chamber. Our mill was one solid plastic casing, so it couldn’t be taken it apart for cleaning. I chose to clean it between every sample by wiping the chamber with a tissue moistened with acetone.
I routinely keep my hand on the lid of these inexpensive mills during operation (a lesson some contestants on “Chopped” could learn). After about a half dozen or so samples, I could feel the pressure starting to build, and then the lid popped off the mill in a kind of a mini-explosion. Evidently, this was loud enough that the personnel in the laboratories on either side of mine came running into my laboratory. Of course, I was wearing my lab coat and safety glasses. Apparently, a white powdery mix of Pringles and diatomaceous earth covered my hair and face. After ascertaining that I was fine, laughter ensued.
While to this day, we’re not entirely sure what happened; the likely cause was either acetone vapors or very fine particulates from the grinding that got down into the motor, causing the small explosion.
The lesson from this case study is to know your process—specifically in this case, the process being not only how the mill works, but how you’re going to clean it. Similar to the “strike anywhere matches” example, don’t overlook things that seemingly are simple.
Case Study #5: A Matter of Scale
On another occasion, our laboratory needed to wash or extract a piece of fabric about the size of the bath towel in boiling or, at least, hot ethanol. Because I had a meeting at one of the other technical centers, I asked our newer technician if she could perform this task. Being fairly new to the laboratory, she looked around for something that would be big enough to hold the fabric and the appropriate amount of solvent. The only sizeable container she could find was a developing chamber for thin-layer chromatography (TLC). She proceeded to place the TLC chamber on a hot plate in the fume hood, put the fabric in the chamber, cover it with probably one to two liters of ethanol, and turn on the hot plate. As things were heating, she needed to walk down to the stockroom to get some other materials.
Meanwhile, the second technician was in the laboratory working at his desk, and noticed flames emanating from the fume hood. He dutifully activated the fire alarm, and then noticed that the TLC tank had a crack in it, causing the liquid ethanol to dribble down the tank onto the hot plate, where it caught fire. He grabbed the fire extinguisher, and put out the fire before the building was completely evacuated. Again, I was off-site and this was before cell phones were prevalent, so I knew nothing about this until the next day, when I returned to the laboratory and was called into a meeting with my boss, the associate director.
Most of our common laboratory glassware is Kimax, Pyrex, or some other type of borosilicate glass. This material has a low thermal expansion coefficient and is designed for heating, because it is resistant to thermal shock. Common glass, like TLC chambers, is soda lime or other “soft” glass that is not meant for heating. When I was an undergraduate, I seem to remember having lessons in bending glass tubing and a little bit of elementary glassblowing and glassware safety training, so I learned about the difference between types of glass. These days, this is not taught, so the appropriate experience is necessary to gain this knowledge.
My associate director asked if we had completed a job safety assessment for this task. My reply was that this was not a new procedure; chemists have been heating organic solvents on hot plates for decades. His claim was that the scale was new or, at least, new to our laboratory.
The lesson from this case study is to perform a job safety assessment, even if it is for a process with which you are familiar, if it is performed in a different manner. It is also important to consider our onboarding and training programs we offer new employees and students in our laboratories: What knowledge do we assume that they have? When preparing a job safety assessment, break down the process to the component tasks, enumerate the risks associated with each task, along with the severity and likelihood of each risk. Details on job safety assessments are found on the internet if your organization does not offer specific training.
Case Study #6: The Only Time
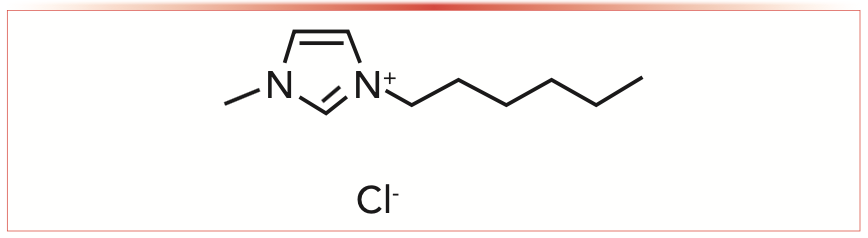
For the past 15 years or so, part of our research program has dealt with bioprocessing—that is, converting biomass from plants to materials and energy. Key to this is to separate the major components (cellulose, hemicellulose, and lignin) from each other. This is not an easy process; plants aren’t readily soluble in conventional solvents. This led us to our foray with ionic liquids. For those less familiar with ionic liquids, one example that was most relevant to our research is 1-butyl-3-methylimidazolium chloride (BMIM Cl), shown schematically in Figure 3.

FIGURE 3: Structure of a typical ionic liquid, 1-butyl-3-methylimidazolium chloride (BMIM Cl).
When our first order of BMIM Cl arrived, a graduate student and two of her fellow students came to my office. To this day, in my entire career it’s the only time I’ve ever had someone come into my office with the Safety Data Sheet (SDS) (formerly Material Safety Data Sheet [MSDS]) and say, “Are you sure you want us to work with this material?” The former MSDS sheets were not as harmonized as the current SDS forms. The MSDS that came with the BMIM Cl looked like is was prepared by a team of lawyers working with a team of toxicologists. The MSDS had copious descriptions of acute and chronic toxicity, aquatic toxicity, warnings, and danger statements.
We have to keep in mind that with toxicity, it really depends on the route of exposure, and we only have three primary routes of exposure—oral, dermal, or inhalation. One of the advantages of ionic liquids is that they’re nonvolatile, so we don’t have to worry about the inhalation hazard, especially if we work in the fume hood. We don’t eat in the laboratory, so we don’t have to worry about oral exposure. We wear lab coats, gloves, safety goggles, and other personal protective equipment (PPE), so dermal exposure is minimized.
Our lessons with this case study are to know your reagents, and read the SDS when you order new materials. Follow the appropriate safety practice. We’re the ones as professional chemists that must deal with the consequences of the compounds we work with, yet most of us have never had a course in toxicology. Perhaps we should be lobbying our local universities to include courses in chemical toxicology in their degree programs.
Case Study #7: Hello, I’m Doug Raynie
This was also in the mid-1990s. For much of my career, I’ve been involved with SFE, generally with carbon dioxide. CO2 is nonpolar, or polarizable. We were interested in extracting triglycerides, or lipids, from foods. Generally, we work at temperatures of at least 80 °C and pressures of 680 atm (or 10,000 psi), or else we add a small amount of an organic cosolvent, such as methanol, for this application. Researchers have been searching for alternative solvents, and literature reports showed some use of nitrous oxide for SFE. Its critical parameters are very convenient to use, similar to that for CO2, which means we can we work at lower temperatures and pressures.
Again, looking to the chemical literature, there were a few reports on supercritical nitric oxide. Each of those reports noted to use caution with nitrous oxide, because it is a strong oxidizing agent. Yet only one of those papers took any special safety precautions to deal with this concern, and another report used nitrous oxide mixed with small quantities of methanol that resulted in a small explosion. I found one paper where a group was using nitrous oxide at 60 °C and reasonable pressures, milder conditions than I used previously for the SFE of lipids from ground coffee beans. I used an unmodified commercial SFE system with vessels that were rated for use at 10,000 psi. Everything worked fine. Being a methodical scientist, I next performed the extractions of the same condition as we did previously with CO2 (80 °C and 680 atm) and, within minutes of starting that extraction, the vessel exploded. You can see the results in the photos in Figure 4.

FIGURE 4 : Photographs of SFE vessel (rated by manufacturer for use at 10,000 psi) explosion caused by use of nitrous oxide during extraction of coffee oils. Reproduced with permission from reference (1).
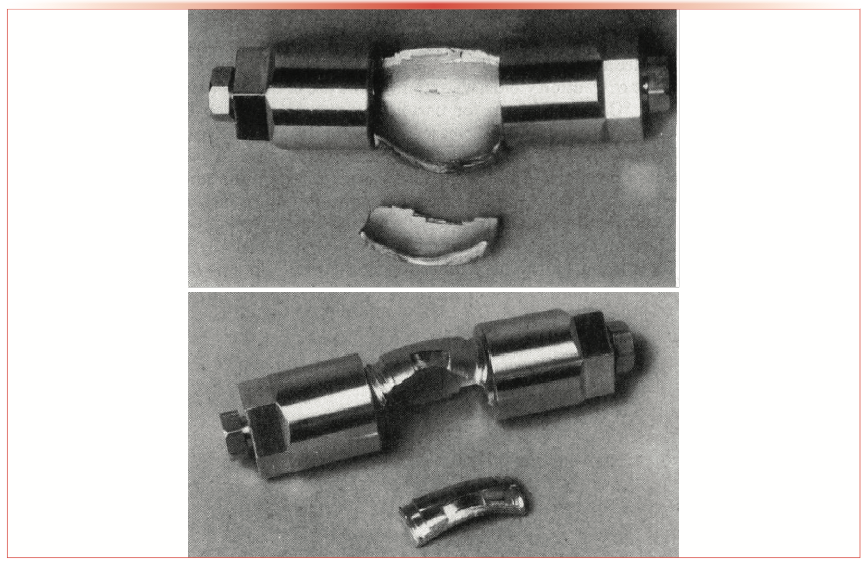
If you look at the bulge in the photo, the vessel split right along the wrench flats and then peeled back along the end caps. The only damage, other than ruining this vessel, was a dent on the inside of the SFE oven. If we think about it, for a fire or explosion to occur, you need an oxidizing agent (nitrous oxide), an organic fuel (the coffee grounds), and some kind of activation energy (provided by free radicals in the coffee grounds). Again, the instrument had minimal damage, and no one was hurt. We did some rough calculations, and determined that the instantaneous pressure inside that vessel was between 80,000 and 100,000 psi. The original tubing to make this vessel, prior to any machining, was rated by the manufacturer to 100,000 psi. There has only been two or three reported instances of catastrophic failure like this on any SFE equipment, at any scale.
Based on this experience, none of the safety features in any commercial SFE, as well as the one paper that they took extra precautions, would not work because the pressure buildup is so instantaneous within the vessel. How do you report this incident, so that no one else would repeat our experience? Keep in mind that, again, this was back in the time before online journals and internet search engines. Typically, laboratory safety incidents were reported in letters to the editor of Chemical & Engineering News, which are not abstracted. So, again, how would people find out about these safety incidences?
We published our experience in Analytical Chemistry (1). I’d like to reiterate what we said there: nitrous oxide should not be used as extracting solvent in SFE, especially with organic samples, and it should not be mixed with organic cosolvents.
This combines all of the previous lessons in this column: Know your system, know your sample, know your process, and know your reagents and solvents. Always think of all the safety considerations, don’t blindly trust what somebody has done in the literature, and think about what are the consequences if something catastrophic happens. I entered this set of experiments with full knowledge of the safety concerns, yet a potentially serious accident occurred.
Now, for the rest of the story.
A few years after this event, I attended a workshop on supercritical fluid processing taught by the Phasex Corporation. Those of you that may be acquainted with Val Krukonis, the owner of Phasex, know that he’s perhaps a bit eccentric. On the first day of the workshop, he arranged a limousine to take the participants to his laboratory. It’s the first day, so we didn’t know each other yet. In the back of the car, there are two groups of conversation and I’m in between those groups, talking to the group in front of me. I then overheard the conversation behind me on high-pressure safety. The person to my immediate right was mentioning work by Doug Raynie at Procter and Gamble with nitrous oxide and a resulting explosion. I simply turned around, offered him a handshake, and said “Hello, I’m Doug Raynie from Procter and Gamble” and then they got the full version of the story.
Conclusions
It was fun to relive the past and tell some stories a little bit different from our typical scientific presentations. I’ve related some of my failures, some of them humorous, some of them with quite serious potential consequences. Keep in mind, we’re all going to make mistakes, regardless of how much attention to detail we have; we just need to make sure to learn from them. As we’re undergoing the planning stages of any of our experiments, we need to make sure to pay attention to every aspect of the analytical process. I hope you have learned from my mistakes.
References
(1) D.E. Raynie, Anal. Chem. 65, 3127–3128 (1993).
ABOUT THE COLUMN EDITOR

Douglas E. Raynie
“Sample Prep Perspectives” editor Douglas E. Raynie is a Department Head and Associate Professor at South Dakota State University. His research interests include green chemistry, alternative solvents, sample preparation, high-resolution chromatography, and bioprocessing in supercritical fluids. He earned his PhD in 1990 at Brigham Young University under the direction of Milton L. Lee. Raynie is a member of LCGC’s editorial advisory board. Direct correspondence about this column via e-mail to LCGCedit@mjhlifesciences.com

")
 Analysis of Hop-Derived Humulone and Isohumulone Constituents in Beer: The Bitter Truth of Hops Utilization During Brewing")









Study Explores Thin-Film Extraction of Biogenic Amines via HPLC-MS/MS
March 27th 2025Scientists from Tabriz University and the University of Tabriz explored cellulose acetate-UiO-66-COOH as an affordable coating sorbent for thin film extraction of biogenic amines from cheese and alcohol-free beverages using HPLC-MS/MS.

Multi-Step Preparative LC–MS Workflow for Peptide Purification
March 21st 2025This article introduces a multi-step preparative purification workflow for synthetic peptides using liquid chromatography–mass spectrometry (LC–MS). The process involves optimizing separation conditions, scaling-up, fractionating, and confirming purity and recovery, using a single LC–MS system. High purity and recovery rates for synthetic peptides such as parathormone (PTH) are achieved. The method allows efficient purification and accurate confirmation of peptide synthesis and is suitable for handling complex preparative purification tasks.



