Drug Development Process: Nonclinical Development of Small-Molecule Drugs


This article provides a high-level overview of the drug development process of small-molecule drugs for the analytical chemist. Emphasis is given to the nonclinical development and roles of the technical development organization in driving the new drug development project from toxicology studies to new product registration. A case study of the career path of a separation scientist is used to illustrate the diversified roles of an analytical chemist in drug development.
New drug development is a multidisciplinary, complex, and expensive process that consists of three stages: basic research, drug discovery, and drug development. This article is the third installment in a series of six overview papers on new drug development for the analytical chemist. The first installment is an overview of the trends and business landscape of the pharmaceutical industry (1). The second installment describes the modern molecular approach to the drug discovery process (2). The third and current article focuses on nonclinical development and the technical development organization, which includes process chemistry, formulation, and analytical chemistry. A case study based on the career of a separation scientist illustrates the varied job functions and career paths in diversified organizations supporting drug development.
Three future installments of the series are planned on these topics: 1) pharmaceutical calculations in a certificate of analysis (CoA); 2) contents of a well-written analytical procedure for regulated testing; and 3) pharmaceutical regulations and guidance. The reader is referred to textbooks (3–4) and short courses (5) for more details on drug development. Valuable informational resources on the roles of the separation scientist in pharmaceutical development are available elsewhere (6–10).
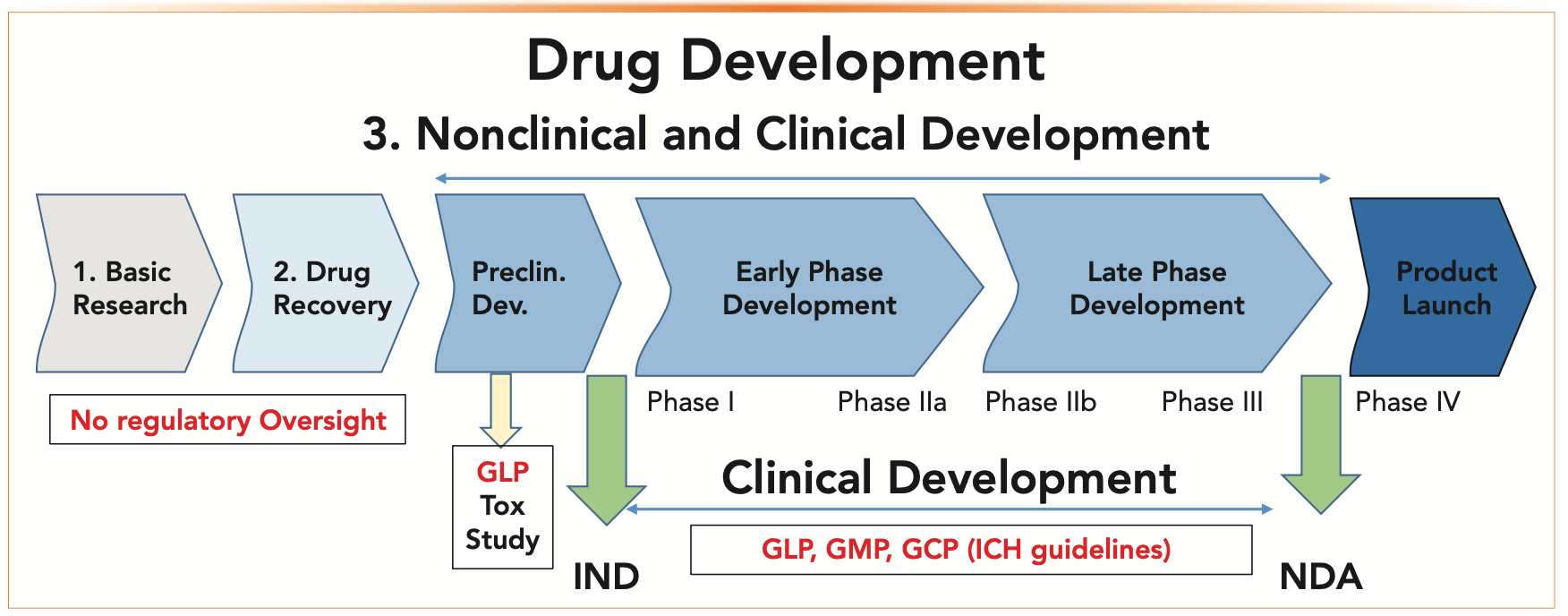
Figure 1 depicts the primary stages in drug development with references to relevant regulations and guidelines. The first two stages (basic research and drug discovery) are described in a previous installment (2). The third stage of drug development can be divided into three substages of preclinical (before investigational new drug (IND) application filing), early-phase (from Phase I to Phase IIa clinical trials), and late-phase development (Phase IIb to new drug application (NDA) registration) (3). Clinical trials in humans commence after the IND filing, and they are supported by nonclinical development, including a technical development or a “Chemistry, Manufacturing and Control” (CMC) organization. CMCs help characterize the drug candidates, develop processes for supplying clinical trial materials (CTM) for both drug substances and drug products, and generate all the necessary technical content for source documents supporting the regulatory dossier leading to the drug approval. There is increasing regulatory oversight as drug development progresses—from minimal oversight in basic research and drug discovery (for example, the Occupational Safety and Health Association [OSHA]) to stringent requirements in late-phase development (for example, in Current Good Manufacturing Practice [cGMP] guidelines). This article focuses on the functions and activities of the technical development organization and the CMC team assigned to each development project.


FIGURE 1: The primary stages of the drug development process and relevant regulations that are associated with each stage.
Glossary and Abbreviations
Table I lists the common terminology and abbreviations associated with small molecule drug development.

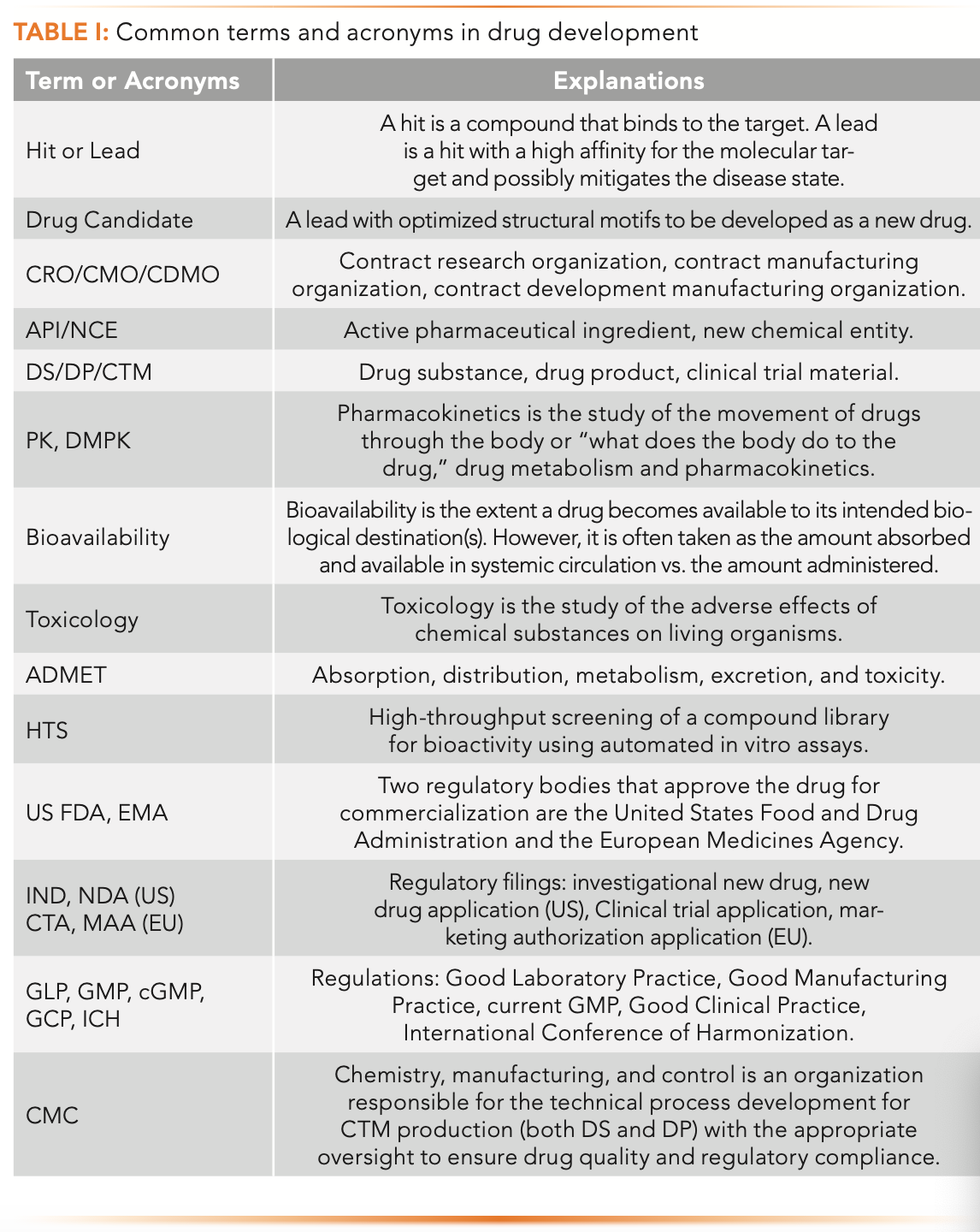
Figure 2 depicts a typical structure of the technical development organization in a mid- to large-sized pharmaceutical company. This includes the pharmaceutical science department responsible for CMC activities and the manufacturing of CTM. This department collaborates closely with other departments, such as drug metabolism and pharmacokinetics (DMPK), pharmacology, safety and toxicology, clinical supply, manufacturing collaboration and outsourcing, project management, and regulatory affairs (8). The clinical quality control (QC) unit can be part of the pharmaceutical science department or a separate unit. Clinical QC is responsible for release testing, setting specifications, and quality assessment functions. Note that organizational design, nomenclature, and functions vary somewhat across the industry.

FIGURE 2: Structure for a technical development organization in a mid-to-large-sized pharmaceutical company, including the groups of the chemistry, manufacturing, and control (CMC) or the pharmaceutical science unit that is responsible for manufacturing the clinical trial material (CTM). * Analytical chemists typically fill these roles. In most companies, drug development is driven by a core project team staffed by scientists from the technical development organization. Each scientist is assigned to one or more project teams.
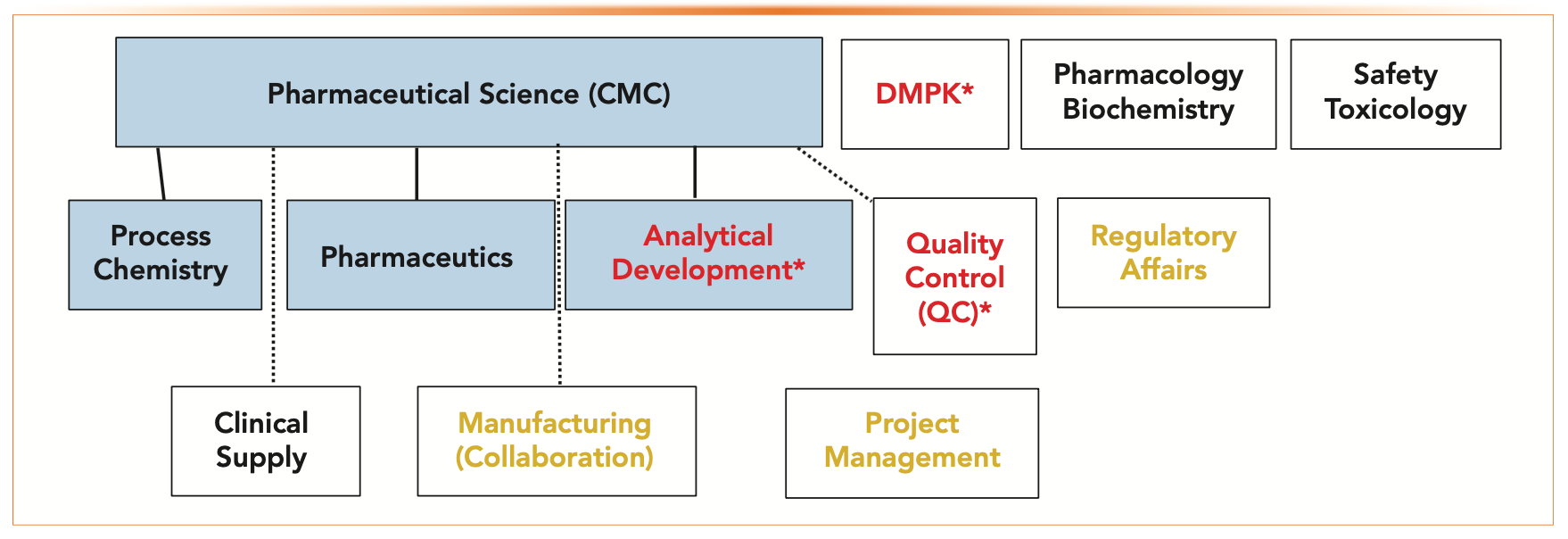
The pharmaceutical science department typically consists of process chemistry, pharmaceutics (formulations), and analytical chemistry, whose roles and functions are described later.
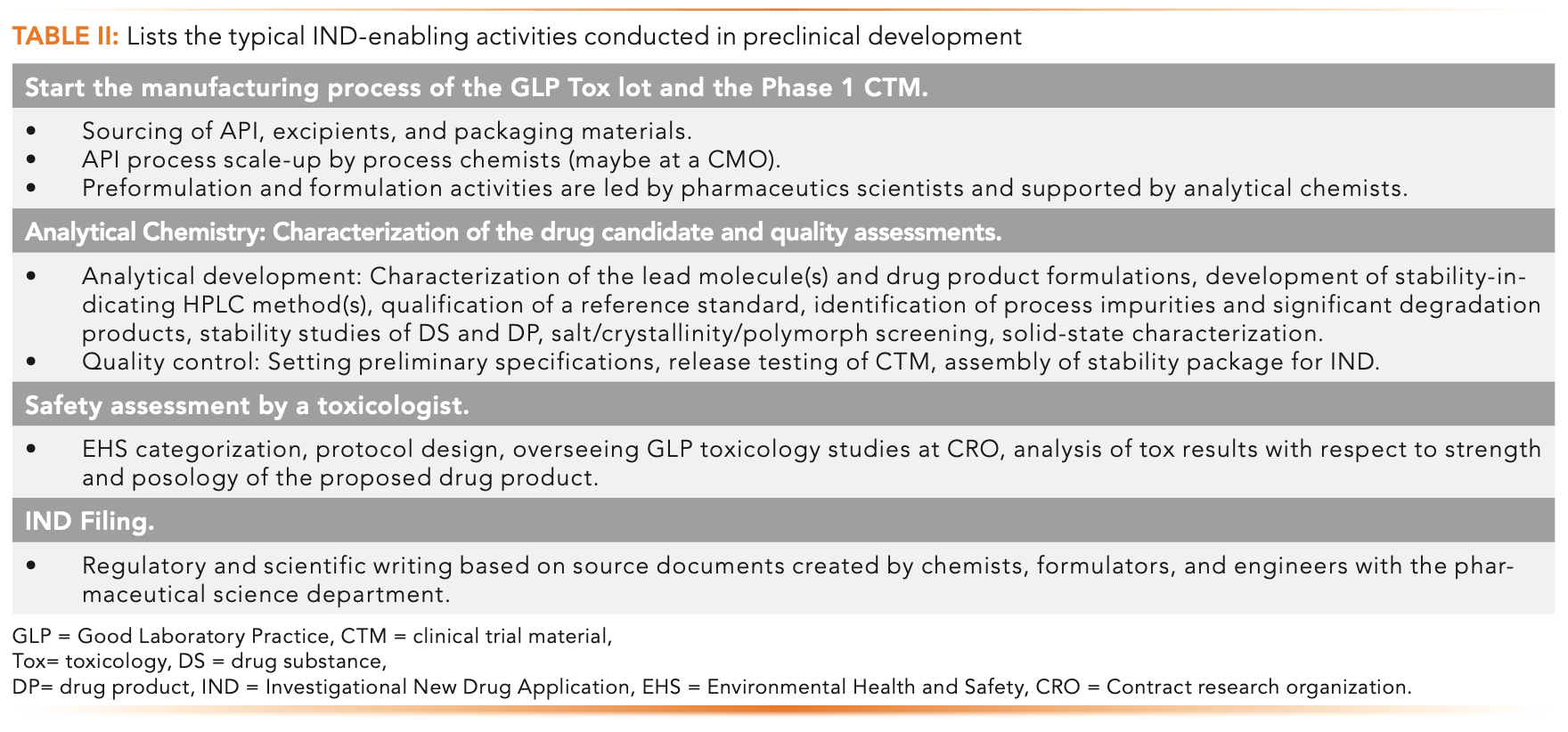
Preclinical Development: IND-Enabling Activities and the CMC Project Team
The drug discovery process ends when the medicinal chemists and their management decide that the leading compound is ready for development (2). The preclinical development phase is led by toxicology (but supported by chemists, analysts, and formulators) and performed on animals and cell lines to establish the safety, tolerability, and dose range predictions in humans for the molecule. The output from the early toxicology studies and molecule characterization is discussed and potentially triggers a nomination of the molecule for a good laboratory practices (GLP) toxicology study (a $1 million-dollar-plus safety evaluation study in two animal species typically conducted at a contract research organization [CRO]). The GLP toxicology study decision triggers the formation of a multi-functional core project team tasked with completing a myriad of IND-enabling activities. The core team comprises of members from the technical development organization shown in Figure 2, with a central CMC project sub-team leading the efforts to complete all necessary investigations and documentation shown in Table II. The timeline for the IND filing is generally 9–18 months after the drug candidate is nominated.

Nonclinical Development: Roles and Functions of the CMC Project Team
In many pharmaceutical companies, “projects are kings,” because the development of innovative drugs leads to new drug approvals, which is the lifeblood of an organization for revenue growth. Each drug development project is driven by its own multidisciplinary core project team and its CMC sub-team. The technical development organization typically has three sub-groups with scientists and research associates assigned to one or more projects. The functions and responsibilities of each group are described in this section.
1. Process Chemistry: Evaluate and optimize the synthetic routes and process conditions of the active pharmaceutical ingredients (APIs) or drug substances.
2. Pharmaceutics: Pre-formulation activities and all formulation development and process scale-up for the production of drug products for the clinic.
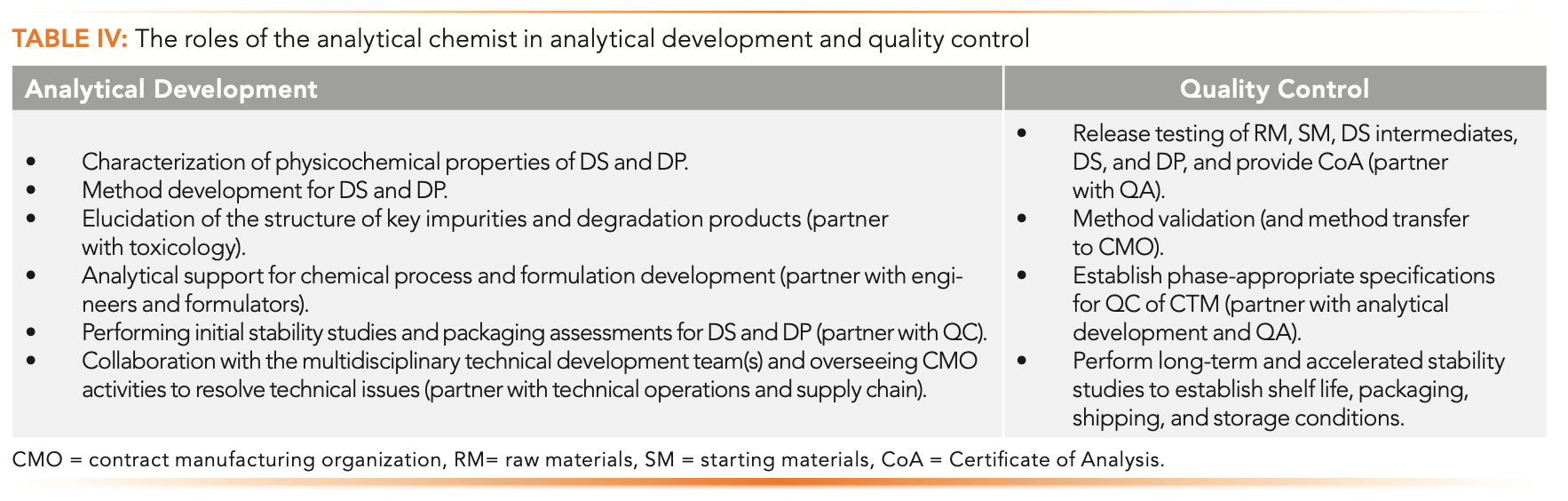
3. Analytical Chemistry: Also known as “Analytical Development.” Develops methodologies to fully characterize and assess the identity, quality, and stability of drug substance and drug product batches, supporting formulation and process development. In some cases, the analytical chemistry group can collaborate with clinical QC or perform all QC functions, such as release testing. These activities are summarized in Table IV.

Process Chemistry: Synthetic Process Scale-up for the Active Pharmaceutical Ingredient (API)
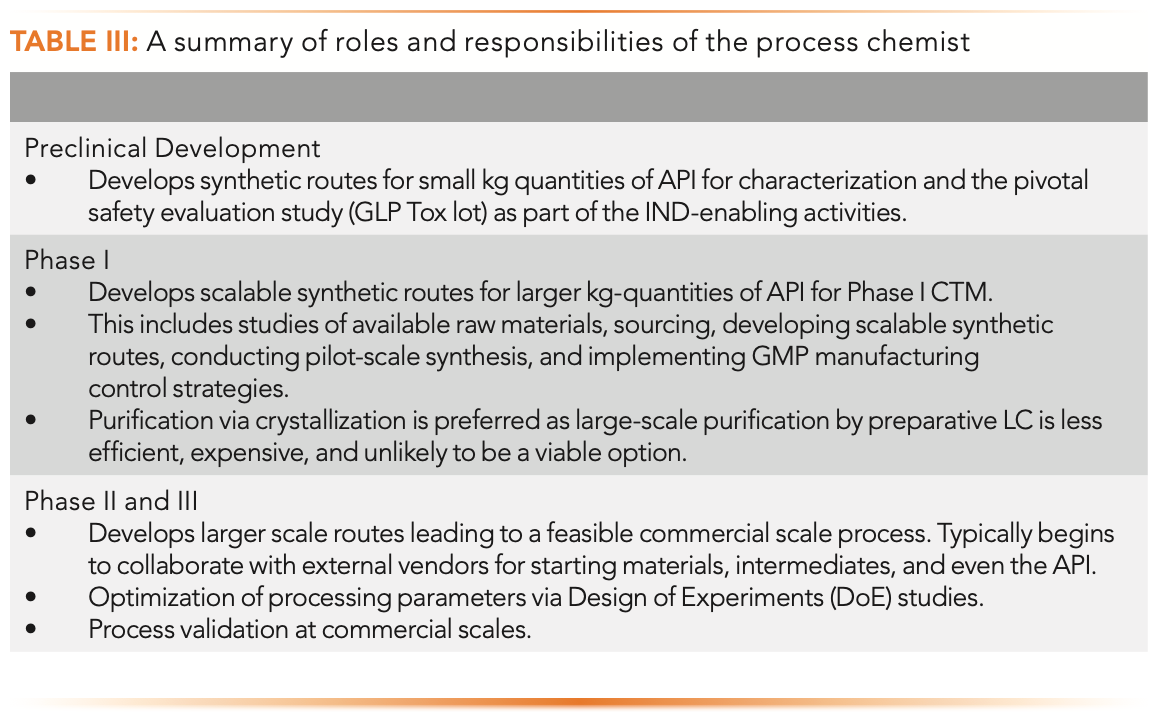
Although the medicinal chemist focuses on the quick synthesis of many leads and optimizes their structure motifs during the drug candidate selection process, the process chemist (also a synthetic organic chemist by training) develops scalable synthetic routes for kg-quantities of the APIs (11). Table III summarizes the roles and responsibilities of the process chemist from preclinical to Phase III.

Pre-Formulation and Formulation
For early-phase in vivo studies, drugs are formulated to maximize exposure to determine safety as well as for easy dispensing, storage, packaging, and stability. Formulators (pharmaceutics scientists) develop simple solutions or suspensions for dosing animals in pilot toxicology and early pharmacokinetics (PK) studies. Formulation strategies are required for determining the route of administration (for example, peroral and parenteral), which also include form selection of the drug substance (salt, crystalline/amorphous, or polymorph) to ensure suitable bioavailability and other desirable physicochemical properties (12).
For Phase I clinical studies, simple enabling formulations are selected, such as solutions, suspensions, or intravenous, and powder in a capsule, formulation in a capsule, or powder in a bottle.
Phase II and III CTM generally uses a more evolved (designed) formulation (although not likely to be the final commercial formulation), which is more complex and requires kg levels of drug substances. Formulation development activities include:
- Excipient selection and compatibility studies, and the development of commercial, scalable drug product formulation
- Multiple packaging configurations and stability studies, including for bulk and non-bulk options
- Drug product process optimization and validation
- Formulators perform drug product development and oversee the production of feasibility, demo, and CTM drug product batches.
For small-molecule drugs, a peroral dosage form (for example, capsules or tablets) is ideal for production, patient convenience, ease of home dispensing, and marketability. A shelf life of two years under room temperature storage is the typical minimum requirement for stability for the packaged drug product. This process is done to ensure that the drug product can be made, packaged, released, shipped, stored, and then prescribed and dispensed to patients to be used for a suitable period.
Detailed Characterization of Drug Candidates
The detailed characterization of the physicochemical properties of lead molecules is required and is typically performed systematically after candidate nomination. The studies are performed by analytical chemists, formulators, DMPK scientists, and toxicologists. The studies typically include several areas.
Chemical
The structure, identity, molecular weight, pKa, solubilities at various pH and solvents, lipophilicity, purity (chemical and chiral), and stability of the molecules are studied.
Physical
The solid-state properties, such as the salt, crystal, and polymorphic forms, hydrate and solvate forms, hygroscopicity, melting or thermal transition points, and particle size distribution are analyzed.
Others
The drug absorption properties (DMPK, ADME), permeability, toxicity for material safety data sheets (MSDS) and environmental, health, and safety (EHS) are also examined.
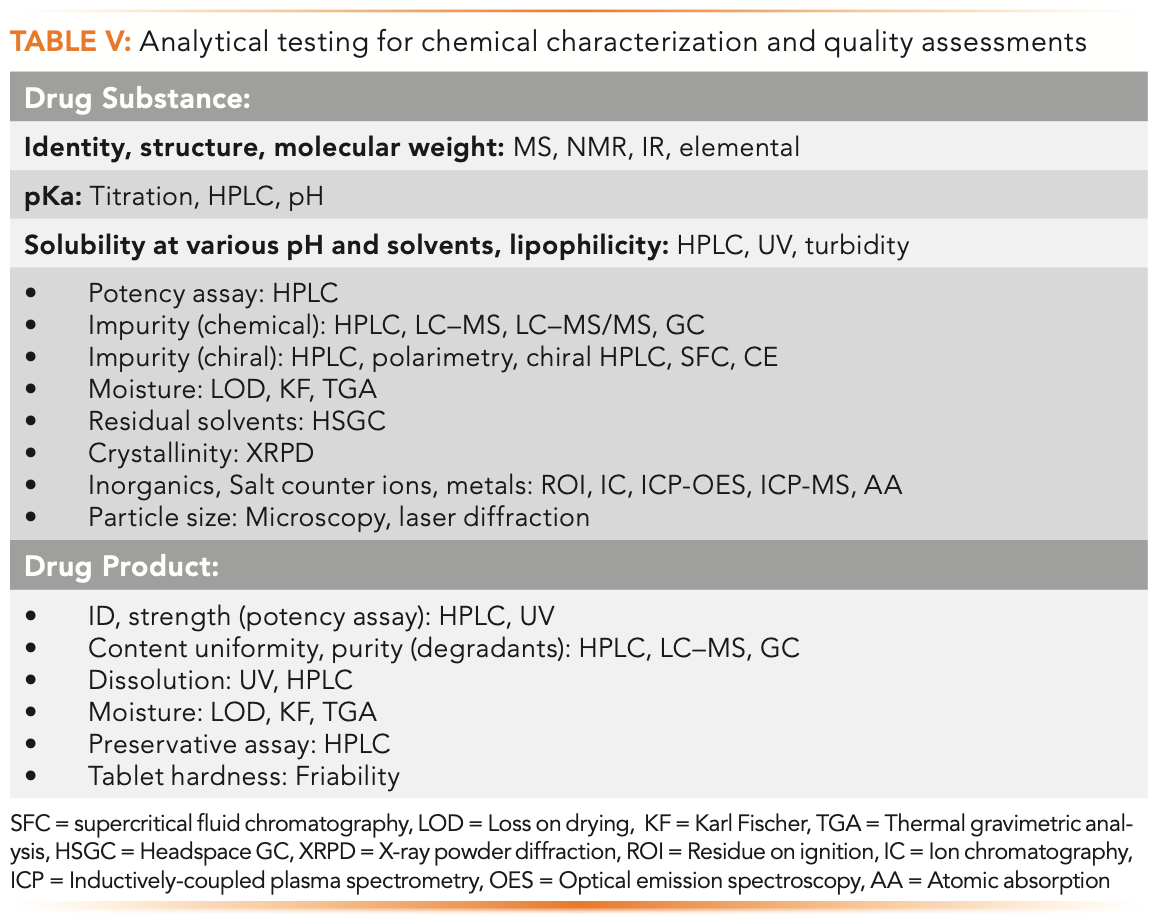
The roles of the analytical chemist in analytical development and quality control are listed in Table IV. The best practice and processes are described further in books and journal articles (6–10). The typical testing and instruments used are listed in Table V.

Case Study: Ingredients in a Lipitor Tablet
The story of Lipitor is a pharmaceutical “fairy tale” that started in 1985 with the synthesis of the molecule by Dr. Bruce Roth, a medicinal chemist at Warner-Lambert who graduated from Iowa State University with a PhD in organic chemistry four years prior. According to Roth, he was discouraged from working on this project because it was a “me-too” drug to lower cholesterol, and there were already five other products on the market. Somehow, he and his manager persisted, and Lipitor became a blockbuster drug because of its superior safety profile. Lipitor became a Pfizer product when Pfizer acquired Warner-Lambert (Park-Davis) in 2000. Lipitor remained the top-ranking drug for 14 years (1996–2011), with a record total sale of $160B until its patent expired in 2011 (1).
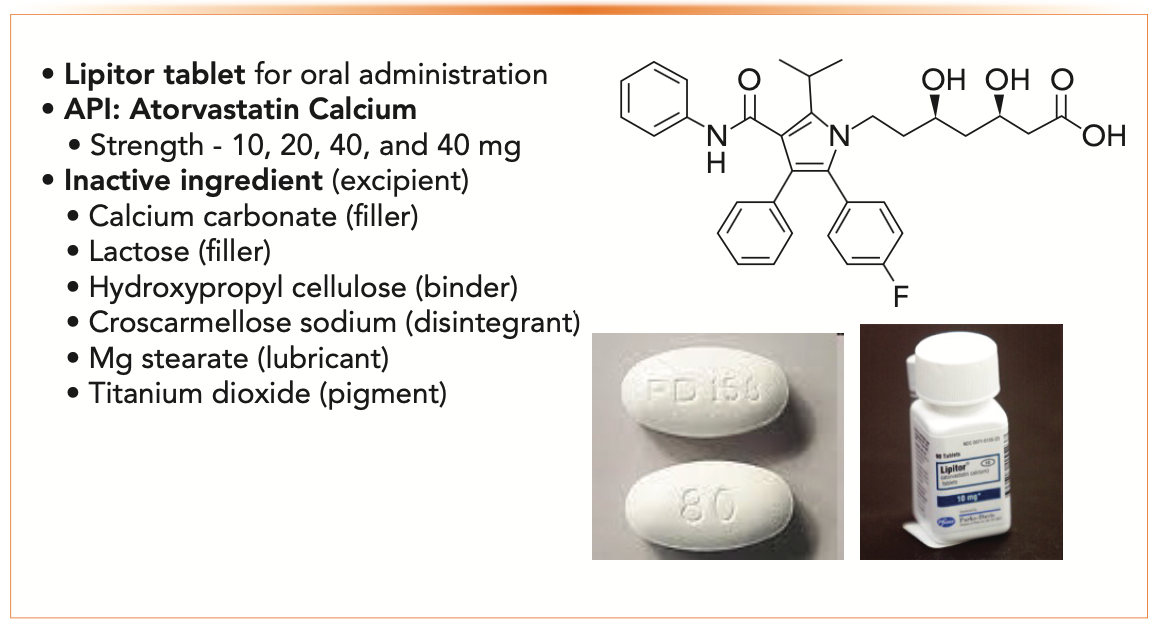
Figure 3 shows the commercial formulation of Lipitor, an oral tablet, and all its ingredients, including the API structure (atorvastatin calcium) and excipients (binder, filler, disintegrant, lubricant, and pigment) (12).

FIGURE 3: Case study: A commercial formulation of Lipitor tablets and their ingredients. Information extracted from an actual package insert of the drug product.
Clinical Development: What are Phase I, II, and III Clinical Trials?
Figure 4 summarizes the goals and typical characteristics of the three phases of clinical trials. The reader is referred to textbooks on clinical trials on the subject for more details (3,13).

FIGURE 4: An overview of clinical trials for Phase I, II, and III clinical testing in humans.
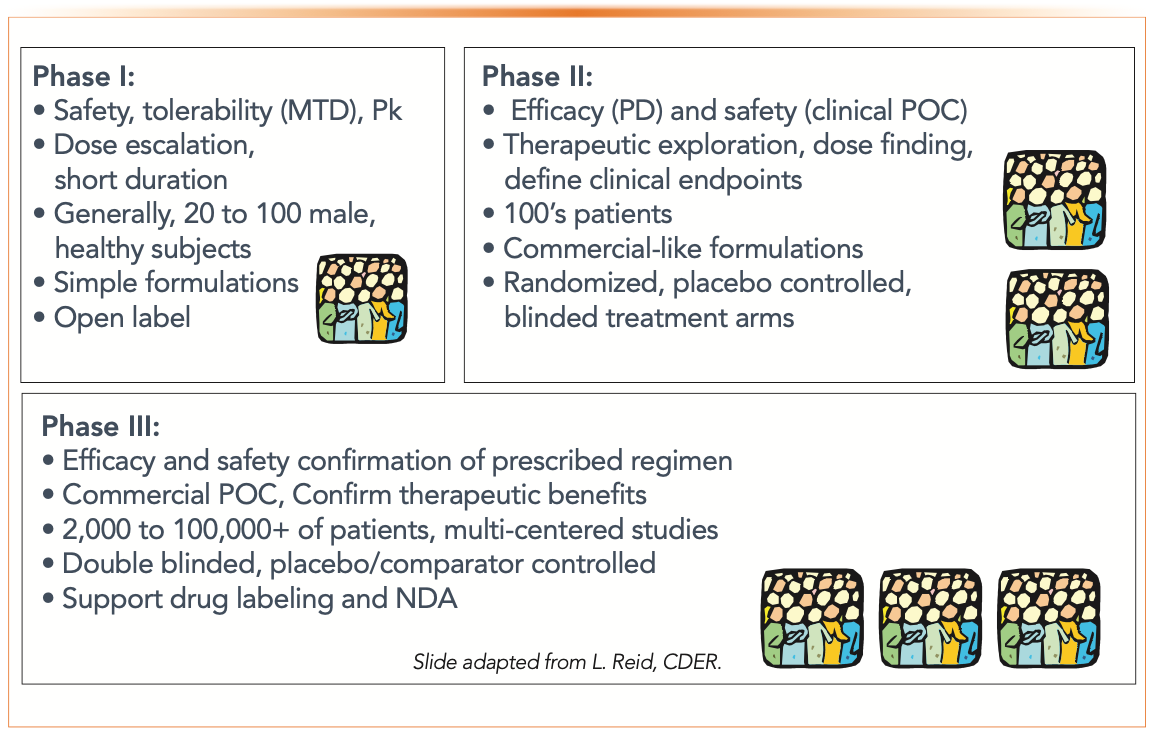
Clinical trials in humans typically commence a month after the filing of the IND. Phase I trials aim to assess the safety and PK of the NCE using dose escalation studies and are performed on healthy volunteers.
In Phase II trials, the goals are dose findings and evaluating the efficacy of the NCE using blinded studies (to establish proof of concept [POC] of the NCE). Phase II studies are completed by using patients with the disease.
Phase III clinical trials aim to establish the commercial proof-of-concept of the dosing regimen using a much larger patient population with near-commercial formulations and scale. Upon the successful completion of the clinical trials, clinical data are analyzed by biostatisticians and clinicians. The data is compiled into the NDA, an extensive document for drug approval submission to the regulatory authorities.
Case Study of an Analytical Chemist in Drug Development
The pharmaceutical industry is the largest employer of analytical chemists, with drug development as the most common job function (1). Although career opportunities vary widely for individuals depending on educational background, timing, location, experience, and leadership and communication skills, this segment offers an attractive career path in terms of pay, benefits, and growth potential.
The case study cited herein is my own journey in drug development, spanning two decades in four different jobs and organizations. I started in drug development late in my career at age 50. Here are some highlights and lessons learned in each job. A complete chronicle of my career as a sep- aration scientist is available elsewhere (14).
Senior Principal Scientist with a Private Pharmaceutical Company in New York (6 years)
My first job in the pharmaceutical industry came from a referral from an ex-colleague in 1999. It came after my first layoff from an analytical instrument company in Connecticut after 19 years. The location of the new job was in Westchester County of New York and did not require relocation. This privately owned company had a successful and approved drug product in pain management and specialized in sustained release drug product development. Because I had extensive experience in high performance liquid chromatography (HPLC), I entered as a senior principal scientist in the pharmaceutical analysis department at its research center. Eventually, I became a research fellow and group leader with six direct reports.
In my first job in the pharmaceutical industry, I learned how to develop stability-indicating HPLC methods and sample analysis under GMP and became a first-time supervisor of professional chemists. Because the company was known for innovative drug product development, formulation scientists drove most development programs.
The company was headquartered in Connecticut and has a manufacturing plant and drug discovery unit in New Jersey. The pharmaceutical analysis department supported the myriad of formulation programs with existing molecules, so there were few CMC or regulatory activities for NCEs. Nevertheless, the combined experience in HPLC and pharmaceutical analysis allowed me to start teaching short courses at national meetings as a subject matter expert and started authoring books and journal articles on these subjects.
Research Director in a CRO in Massachusetts (1.5 years)
My six-year stint with the private company ended abruptly in 2005 when the company lost a court battle on the patent litigation dispute of its flagship product and decided to close down the research center. Because the job market was weak that year and few pharmaceutical companies were hiring, I accepted a job 180 miles from my Connecticut home in a start-up contract laboratory in Cape Cod, Massachusetts, as a research director. For 18 months, we stayed in a rental apartment on weekdays and commuted home every weekend. I served as a study director for ~20 clients’ projects in method development and validation and sample analysis, typically under GLP or GMP regulations for pharmaceutical and consumer products.
I reported directly to the owner of the parent company in Ohio, and we had teleconferences every Monday at 7:30 am to report my weekly job progress. In my time sheets, I accounted for every 1⁄2 hour of my work week assigned to a billable client’s project or a company’s general account. I became very efficient in deliverables and could do a project proposal in 30 min and a study report in a few hours.
Working in a contract laboratory is a challenging experience because having multiple projects from different clients is always a tricky balancing act. We had four Waters Alliance HPLC systems, and I would do most of the method development and sample analysis with assistance from two technicians. As ultrahigh-pressure liquid chromatography (UHPLC) debuted as the first commercial UHPLC system from the Waters Corporation in 2004, I managed to place a demonstration unit in our laboratories in 2006. The weekend commutes and the upkeeps of two homes were difficult for the family and me, so I was ready for a change after a year.
Senior Scientist and CMC Analytical Team Lead in California (8 years)
My stint with the contract laboratory ended soon after an unexpected headhunter’s call for a senior scientist job at a prestigious biotech company in the Bay Area in California. The company had just started a pharmaceutical science department in their new small-molecule drug discovery program and was looking for an experienced separation scientist with a strong publication record. I went for an interview in December 2006 and started working in South San Francisco in March 2007.
This job change worked well, with challenging projects and tremendous learning opportunities on CMC, drug development, mass spectrometry (MS), quality control, and regulatory filings. I stayed there for eight years and worked on four drug development projects (three small molecules projects and one antibody–drug conjugate project). My primary project was an AKT inhibitor with three chiral centers for oncology indications. I stayed on this project for five years, taking the molecule from Phase 0 to Phase IIb. Serving as the analytical lead in the CMC team was intense because the role involved weekly project meetings and many teleconferences with numerous contract manufacturing organizations (CMOs) while supervising internal studies by research associates. During my fifth year, the analytical development group merged with the clinical QC unit, which meant that release testing and GMP stability testing also became my responsibility.
The company encouraged its scientists to publish and present at conferences, so I was able to continue both activities and developed a reputation in HPLC and pharmaceutical analysis.
Pharmaceutical Consultant in Connecticut (8 years)
I left California in 2015 and returned to Connecticut to be closer to my family. I became a pharmaceutical consultant focusing on HPLC training, authoring books and articles, and CMC consulting (method development and validation, drug quality, and regulatory filings). Life as a self-employed consultant is simpler, with no commuting, group meetings, or management responsibilities. All consulting was virtual, and contract development and manufacturing organizations (CDMOs) performed the experimental studies I managed. Marketing and obtaining new clients can be most challenging for new consultants. I was fortunate to get clients from a vast professional network on LinkedIn and prior contacts from teaching and speaking at conferences and publishing journal articles and books. I would travel 8–10 times yearly to conferences and clients until the pandemic shut down in March 2020. Hopefully, both travel and business will return to normal soon.
The Covid-19 pandemic dragged on for over two years and adversely impacted the global economy and many industries. It also created a shortage of experienced analytical chemists in the booming pharmaceutical industry. I am convinced that the job market outlook for analytical chemists will remain strong for decades to come.
Summary
This article provided a brief overview of the drug development process and the functions of the technical development organization and the CMC project team. A case study based on my career was included to illustrate the roles played by the separation scientist in supporting drug development as a laboratory scientist, analytical CMC project team lead, study director at a CRO, and self-employed pharmaceutical consultant.
Disclaimer
This paper provided a high-level overview of the nonclinical drug development process and the role of the technical development organization. The information presented here stems from books, journal articles, and internet resources collected for my short course on the drug development process (5), and it often reflects my personal perspective and experience as an analytical chemist. Presenting a concise primer in a few thousand words on this complex and diverse process is challenging. The figures and tables in this article are used to anchor descriptions in texts and are supported by the citations of books and articles as key references. Some duplications from the previous installment on the drug discovery process are intentional (such as in the table of terminology and the discussion about clinical development) to keep the article as a single, self-contained document for better flow and clarity.
Acknowledgments
The author thanks the following reviewers for providing timely comments on the technical content and clarity of the manuscript: Alan McKeown from Vertex; Leon Doneski from Arcutis Biotherapeutics; Parvinlal Saraswal from Moderna; Alice Krumenaker from Hovione; Samer Sansil from Moffitt Cancer Center; Mike Shifflet from J&J Consumer Health Care; Jenny Lin Gao of Tergus Pharma; and Stanislav Bashkyrtsev from Elsci. Their prompt responses are deeply appreciated for improving the accuracy and clarity of the article.
References
(1) M.W. Dong, LCGC North Am. 40(6), 252–257 (2022).
(2) M.W. Dong, LCGC North Am. 40(8), 344–350 (2022).
(3) R.G. Hill and H.P. Rang, Eds., Drug Discovery and Development: Technology in Transition (Churchill Livingston, Edinburgh, United Kingdom, 2nd ed., 2012), Chapters 4–11.
(4) B.E. Blass, Basic Principles of Drug Discovery and Development (Academic Press, New York, NY, 1st ed., 2015).
(5) M.W. Dong, “Drug Discovery and Development Processes,“ Pittcon 2019 short course presented at Pittcon, Philadelphia, PA, 2019.
(6) S. Ahuja and M.W. Dong, Eds., Handbook of Pharmaceutical Analysis by HPLC (Elsevier/Academic Press, Amsterdam, The Netherlands, 2005).
(7) Y.V. Kazakevich and R. LoBrutto. Eds., HPLC for Pharmaceutical Scientists (Wiley, New York, NY, 2007).
(8) M.W. Dong, HPLC and UHPLC for Practicing Scientists (Wiley, Hoboken, NJ, 2nd ed., 2019), chapters 9 and 10.
(9) M.W. Dong, LCGC North Am. 33(10), 764–775 (2015).
(10) D. Kou, L. Wigman, P. Yehl, and M.W. Dong, LCGC North Am. 33(12), 900– 909 (2015).
(11) K. Gadamasetti and T. Braish, Eds., Process Chemistry in the Pharmaceutical Industry: Challenges in an Ever Changing Climate (Taylor and Francis, New York, NY, 2020).
(12) G.D. Tovey, Pharmaceutical Formulation: The Science and Technology of Dosage Forms (RSC Publishing, Cambridge, United Kingdom, 2018).
(13) L.M. Friedman et al, Fundamentals of Clinical Trials (Springer, New York, NY, 5th ed., 2015).
(14) M.W. Dong, My Career as a Separation Scientist (Kindle Direct Publishing, Seattle, WA, 2021).
ABOUT THE AUTHOR

Michael W. Dong is a principal of MWD Consulting, which provides training and consulting services in HPLC and UHPLC,method improvement, pharmaceutical analysis, and drug quality. He was formerly a Senior Scientist at Genentech, a Research Fellow at Purdue Pharma, and a Senior Staff Scientist at Applied Biosystems/PerkinElmer. He holds a PhD in Analytical Chemistry from City University of New York. He has more than 130 publications and a best-selling book in chromatography. He is an editorial advisory board member of LCGC North America and the Chinese American Chromatography Association. Direct correspondence to: LCGCedit@mmhgroup.com.



")


















