Separation Science in Drug Development, Part IV: Quality Control
LCGC North America


This fourth and last installment in the series of “Separation Science in Drug Development” provides an overview of modern practices of Quality Control in small molecule drug development including activities such as setting specifications, method validation/transfer, release and stability testing, and authoring CMC sections of regulatory filings.
This fourth and last installment in the “Separation Science in Drug Development” series provides an overview of modern practices of quality control in small-molecule drug development, including activities such as setting specifications, method validation and transfer, release and stability testing, and authoring chemistry, manufacturing, and controls (CMC) sections of regulatory filings.
Quality control (QC) in the pharmaceutical and biotech industry is part of current good manufacturing practices (cGMP) and an overall quality system, and is regulated by the United States Food and Drug Administration (US FDA) and health authorities around the world (1–5). Quality is defined in the following context by the FDA as follows: “Every pharmaceutical product has established identity, strength, purity, and other quality characteristics designed to ensure the required levels of safety and effectiveness. . . . The phrase achieving quality means achieving these characteristics for a product” (6).
QC should not be confused with quality assurance (QA); both are parts of the “Quality Unit” in cGMP terminologies. The FDA makes the following statement (6):
QC usually involves (a) assessing the suitability of incoming components, containers, closures, labeling, in-process materials, and the finished products; (b) evaluating the performance of the manufacturing process to ensure adherence to proper specifications and limits; and (c) determining the acceptability of each batch for release. QA primarily involves (a) review and approval of all procedures related to production and maintenance, (b) review of associated records, and (c) auditing and performing/evaluating trend analyses.
The International Conference on Harmonization (ICH) of Technical Requirements for Registration of Pharmaceuticals for Human Use was founded in 1990 by the regulatory agencies and industry associations in the European Union (EU), United States, and Japan (7). It has published extensive guidelines governing the quality (Q), safety (S), efficacy (E), and multidisciplinary (M) requirements for product registration. The ICH guidelines are widely recognized by health authorities and the industry in these three regions of the world. QC for small molecule chemical drugs is covered by the quality (Q) guidelines: Q1 for stability, Q2 for validation, Q3 for impurities, and Q6 for specifications. Although ICH Q8 and Q11 do not explicitly cover QC, they provide valuable guidance on current expectations for the development of process and product control strategies, including specifications. The ICH guidelines are intended for late-stage development products (phase 3) for marketing applications. During early development (phases 1 and 2a), the ICH guidelines can serve as a reference, but they are not intended to be applied directly without assessment of their appropriateness for the phase of development. The FDA guidance for industry on cGMP for phase 1 investigational drugs has a section for QC but does not delve into significant details (8).


The International Consortium on Innovation and Quality in Pharmaceutical Development (IQ Consortium) was formed in 2010 by more than 25 pharmaceutical and biotech companies and has expanded to 40 member companies at the time of this writing (9). The mission of the IQ Consortium is to advance science-based and scientifically driven standards and regulations for pharmaceutical and biotechnology products worldwide. The GMPs in Early Development Working Group within the IQ Consortium has held several conferences bringing together industry representatives and FDA officials. Summaries from these meetings have been published as a series of position papers on drug product manufacturing, specifications, validation, and stability for early development (10–14). Some of the important discussion points on QC in the papers are referenced and highlighted in this article.
The roles and responsibilities of the analytical chemist working in QC generally include setting specifications; method validation; testing of starting materials, raw materials, and intermediates in process control; release testing of drug substances and drug products; stability testing and setting retest date and shelf life; method transfer (if applicable); and authoring of regulatory filings. Many of these activities are closely related and impact one another. The scope of each activity varies depending on the stage of development. In this article, we discuss the key QC activities in early and late-stage development with the emphasis on the former, as the latter is well covered by the ICH guidelines. Readers are encouraged to use the referenced literature to pursue further understanding of the individual topics.
Setting Specifications
A specification is defined in ICH Q6 as “a list of tests, references to analytical procedures, and appropriate acceptance criteria, which are numerical limits, ranges, or other criteria for the tests described . . . Specifications are critical quality standards that are proposed and justified by the manufacturer and approved by regulatory authorities as conditions of approval” (15). Under cGMP, the QA approved specifications and analytical methods must be in place before clinical lots of drug substances or drug products can be released. Some companies do not set formal release specifications for starting materials of drug substance in early development. The starting materials are tested for characterization and information gathering, but their acceptability is decided by use test results instead of against formal specifications (12).
The analytical chemist plays a leading role in setting specifications. Generally, the analytical chemist and process chemist (for drug substance) or formulation scientist (for drug product) propose the specifications based on the physicochemical properties of the drug substance and drug product and knowledge gained from process and product development. The specifications are then discussed within the technical development team including members from QA and regulatory affairs. The final specifications are typically endorsed by the technical team and management.
Specifications should be appropriate for the phase of drug development. In early development, especially in phase 1, drug substances and drug products are often manufactured using processes that are not optimized. With limited manufacturing and testing experience and incomplete understanding of critical quality attributes (CQA), critical process parameters (CPP), and critical material attributes (CMA) (1), it may be unrealistic or even counterproductive to try to develop a tight control of these early processes that are likely to change in late development. Phase 1 and 2a trials aim to assess the safety, tolerability, pharmacokinetics (PK), and early signs of efficacy of the drug candidate, and typically have short dosing durations and a small number of subjects. Specifications at this stage should support the clinical goal of safety assessment, while allowing flexibility to gather more information about the product to justify meaningful specifications in late development.
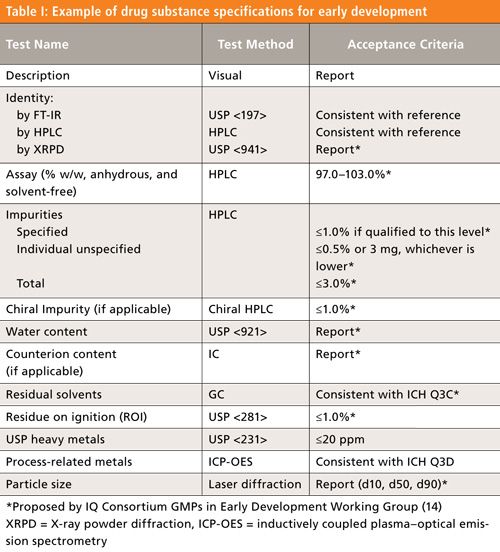
Tables I and II are examples of drug substance and drug product specifications proposed by the IQ Consortium for early development (14). It is recognized that individual companies have different risk tolerances in setting specifications. Nevertheless, the specifications proposed by the IQ Consortium can serve as a good starting point towards more consistency in setting specifications for early development. As shown in the tables, impurity levels higher than the ICH limits may be considered acceptable for drug substances and drug products in early development, based on limited drug exposure in trials of short duration and small size. It may be appropriate to use “Report” for water content and counterion content until sufficient data have been obtained to justify a meaningful specification limit. Similarly, “Report” may be acceptable for dissolution specifications in early development.
In early development, simple formulations such as active pharmaceutical ingredient (API) powder in capsules (PIC) might be used to save time and cost for formulation development if feasible. PIC are typically manufactured by automated equipment that records the content weight of each and every capsule filled in the batch and rejects the units that fall outside a predetermined acceptable weight range. This 100% in-process control provides a high level of assurance of content uniformity, and it can serve as a justification for waiving the uniformity of dosage units (UDU) test by weigh variation (WV) or by content uniformity (CU) (typically a high performance liquid chromatography [HPLC] test) on the finished product.
In general, more-flexible impurity limits for oncology products may be justified based on the nature of the disease and the risk-to-benefit balance for the subjects enrolled in phase 1 trials (that is, cancer patients instead of healthy volunteers).
A general expectation is that specifications will be tightened as the development progresses through early and late stages. Late-stage product specifications generally follow the ICH guidelines. Table III lists the current ICH guidelines on specifications and impurities in new chemical entities (NCE).


Risk assessments and technical evaluations should be conducted as part of control strategy development, including specifications. ICH Q6A includes a number of decision trees to evaluate specifications for specified impurities, polymorphism, enantiomeric impurity, dissolution, particle size, and microbial limits (15). Here, let’s discuss a few examples. A risk assessment may be conducted on the potential for microbial contamination and proliferation in nonsterile, oral solid dosage forms, for example, by evaluating the following factors. The drug substance is typically crystallized or isolated from organic solvents in the final step of synthesis and dried at an elevated temperature. Such an environment and process have low potential for introducing microbial contamination. Commercially available excipients are generally tested for microbial activity per compendial requirements (for example, United States Pharmacopeia [USP] <61> and <62>), and results are documented in the excipient manufacturer’s certificates of analysis (CoAs). These “clean” excipients reduce the risk of microbial contamination. The manufacture of clinical trial materials (CTM) is typically conducted in cGMP clean rooms with high-efficiency particulate air (HEPA) filters that have low potential for introducing microbial contamination. The water activity of the drug product is critical for evaluating the microbial proliferation potential in the packaging configurations under long term storage conditions, as described in USP
<1112> (16). Water activity below 0.6 does not support microbial growth (16). Storage with desiccant also reduces the water content and water activity of the drug product. All of these factors can be used to justify a reduction or waiver of microbial limits testing for the drug product.
According to the latest FDA draft guidance for industry (17), for drug products in biopharmaceutical classification system (BCS) classes 1 and 3 (high solubility drugs) (1), if the product meets a dissolution specification of Q = 80% in 15 min, the USP disintegration test with a specification limit of within 5 min (in 0.01 M hydrochloric acid) may be used to replace dissolution testing for routine release and stability. However, the approved dissolution method should be retained as the primary method in the specifications and the approved disintegration method used as an alternate method (17).
Controlling Genotoxic Impurities
Controlling genotoxic impurities (GTIs) in pharmaceutical products has been a hot area of discussion in recent years, and it has attracted a lot of attention from regulatory authorities and the industry (18,19). GTIs need to be controlled at very low levels, and the analyses of GTIs often rely on hyphenated techniques such as liquid chromatography–mass spectrometry (LC–MS) or gas chromatography (GC)–MS to achieve high specificity and sensitivity. Controlling GTIs is not the same as specifying and testing an impurity in the final product. In fact, applying control upstream in the synthetic process or relying on chemical fate reasoning by demonstrating the purging power of the process itself (through spike-purge studies) is generally preferred over specifying and testing GTIs in the final product (19).
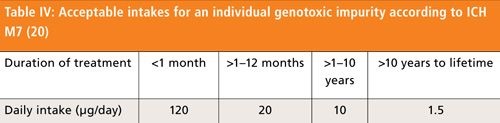
Regulations on genotoxic impurities have evolved over the years since the first regulatory guideline was published in 2003. The latest and most significant development in the area was the publication of ICH Guideline M7 in June 2014 (20). A few important changes brought about by ICH M7 are worth highlighting. The acceptable intakes for a genotoxic impurity in relation to less-than-lifetime (LTL) exposure have been revised to higher limits (Table IV) than allowed by the previous FDA and European Medicines Agency (EMA) guidelines.

Another important change per ICH M7 is that for phase 1 clinical trials of up to 14 days, impurities containing structural alerts (class 3) (18) can be treated as nonmutagenic impurities, and would not trigger an action for further assessment (such as Ames testing).
Method Validation
The scope of method validation as well as the appropriate validation parameters and acceptance criteria depend on the type of analytical methods and the phase of development (21). Compendial methods do not need to be validated, but should be verified for their suitability under actual conditions of use (22). Noncompendial methods, typically chromatographic methods developed for assay and impurities, residual solvents, content uniformity, and dissolution, should be properly validated for the release and stability testing of drug substances and drug products (23–25). Method validation in late development is expected to follow ICH Q2 requirements (26). In early development, validation generally applies to methods used for release and stability testing of the drug substance and drug product. Methods for the analysis of raw materials, starting materials, intermediates, and in-process control need to be evaluated and “qualified” to be scientifically sound and suitable for its intended use, but do not require full, formal validation at this stage of development.
Successful method validation relies heavily on the quality of method development. It is prudent to perform at least an evaluation of method recovery before formal validation to ensure that the method is indeed “validatable” (24). For a drug product, recovery and stability during sample preparation should not be taken for granted. Sample preparation procedures for the drug product are often different from those for the reference standard and drug substance. Selection of a suitable diluent for the drug product is critical to ensure adequate recovery, stability of the drug, and diluent compatibility with the mobile phase (27). Special attention should be paid to excipients that may cause interference or degradation during sample preparation. For example, fumaric acid, with its conjugated double bonds, has a good ultraviolet (UV) chromophore. If used as an excipient, it will appear as a peak in the HPLC–UV chromatogram. Fumaric acid can also react with methanol (if used in the diluent), forming an ester that can appear as an additional peak of random size depending on how long the sample solution is stored after preparation before analysis. Therefore, in such cases, acetonitrile is preferred over methanol to avoid the esterification of fumaric acid. Fumaric acid may also cause API degradation during sample preparation, especially when heat and sonication are applied to an aqueous solution. A diluent containing a lower amount of water may be needed in this case to minimize degradation. However, if this diluent is too strong for the HPLC mobile phase, a subdilution step with a weaker diluent compatible with the HPLC method may be necessary to avoid peak distortion. Issues like this, if not discovered and addressed during method development and evaluation, can cause failure to meet acceptance criteria during method validation (27,28).
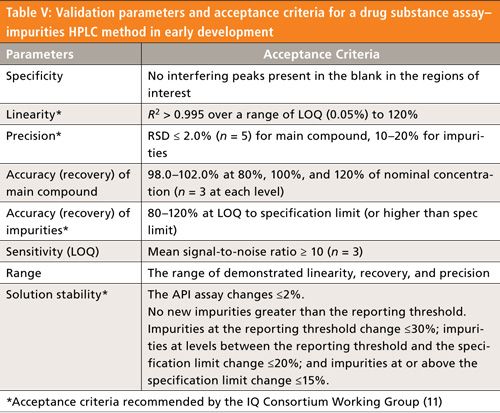
Table V is a summary of typical validation parameters and acceptance criteria for a HPLC method for drug substance identification, assay, and impurities in early development (11). Parameters such as intermediate precision and robustness are not required at this stage. Because of the lack of impurity standards in early development, the drug substance is often used as a surrogate for impurities in the accuracy experiment. Since the diluent and sample matrix are the same for reference standards and drug substance samples, linearity and recovery validation experiments can use the same samples. Phase 1 method validation typically does not require a formal validation protocol or report. Certain parameters such as injection repeatability and sensitivity can be obtained from the system suitability test in a HPLC run, and they may not need to be repeated again as part of the method validation experiment.

Method Transfer
The need for method transfer may arise, when drug substance and drug product manufacturing and testing is outsourced to a contract manufacturing organization (CMO), or when technical handoff occurs between different functions within the same company, especially for larger, global companies with separate early and late development organizations and multiple sites (23). Before analytical testing for GMP samples can be performed at a different company or site, some form of technical transfer is expected. This can be done by method transfer from the originating laboratory to the receiving laboratory, complete method validation at the receiving laboratory, covalidation by both parties, or a transfer waiver. If a method has not been validated and is not anticipated to be used by the originating laboratory, method validation by the receiving laboratory is preferred. Similar to method validation, method transfer typically applies to chromatographic methods developed for each drug substance and drug product. Method transfer is not required for compendial methods, although the laboratory performing the compendial test must demonstrate that it can execute it correctly and that the compendial test is suitable for its intended use.
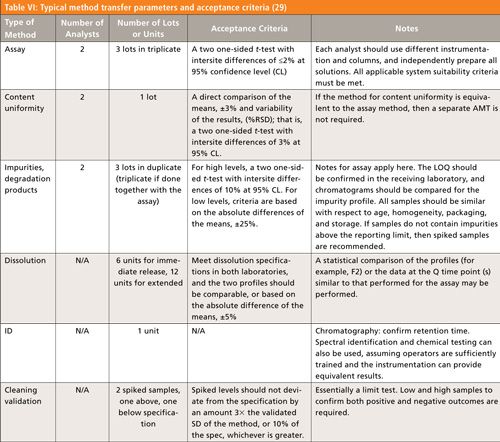
Generally, a method transfer protocol is written by the originating laboratory or company, and approved by QC and QA at both the originating and receiving laboratories or companies. After the method transfer laboratory work is completed, a method transfer report is written by the receiving company, and reviewed and approved by QC and QA at the receiving and originating companies. Table VI gives an example of method transfer parameters and acceptance criteria for late development (29). The method transfer requirements for early development are more flexible than those during late development. For example, it is acceptable to use fewer batches and samples, and wider ranges of acceptance criteria can be justified in early development.

Release and Stability Testing
Quality control does not simply mean testing the final drug substance or product for conformance to specifications. Control points should be based on the understanding of the overall manufacturing process, and applied to key components and critical steps, such as starting materials and intermediates, and during in-process control steps. Controlling at the final product step alone is simply too late or ineffective to assure product quality. Ideally, release testing of the final product serves as a confirmation that it meets specifications rather than being the primary control point of product quality. The principles of quality by design (QbD) have been advocated by the FDA in the last decade and are being adopted by the pharmaceutical industry (30).
Under cGMP, release testing of the drug substance and drug product is conducted per established specifications and methods. The results of release testing are documented in a CoA, which is reviewed and approved by QC and QA. The CoA is a critical document required for QA to release the batch.
Stability testing provides information to demonstrate that the drug substance and drug product are stable under the proposed storage conditions and packaging configurations within its intended use period (31). Stability testing typically uses the same analytical methods as release testing, and is focused on those attributes at risk of changing during product storage. For drug substances, stability testing generally includes appearance, HPLC assay and impurities, water content, chiral impurity, and X-ray powder diffraction (XRPD). Attributes such as identity, residual solvents, residue on ignition (ROI), heavy metals, and process related metals typically do not change after manufacture and are therefore not part of stability programs. For drug products, identity and UDU tests are included for initial release but not for stability.
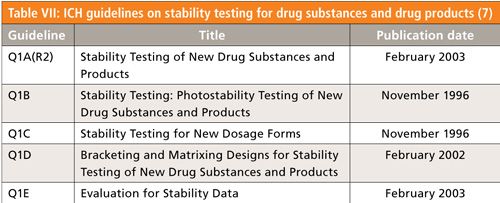
ICH has a number of guidelines on stability testing (Table VII) for commercial product registration, including batch selection, stability conditions, and time points. For new drug application (NDA) filings, 12 months of stability data from three pilot-scale “validation” batches representative of the commercial process are generally required.

The stability testing requirements for early development is less well defined. Before formal stability studies, usually forced degradation studies are conducted to gain a quick understanding of the compound’s stability under various conditions (23,32). Forced degradation studies are also used to study degradation pathways and verify that the HPLC method is stability indicating. The drug substance is subjected to heat in solid state and in solution, stressed in acidic, basic, and oxidative solutions, as well as exposed to UV and visible light in accordance with ICH Q1B requirements (33). For the drug product, excipient compatibility studies are typically done to assess the impact of excipients on drug product performance and stability. In addition, the drug substance and drug product can be exposed to a range of elevated temperature and various humidity levels in a 2–3 week study. Potency and degradant data from such a study can be used to predict shelf-life in different packaging configurations under different storage conditions, using commercially available software. The knowledge gained from these studies is important for the understanding of the conditions (for example, temperature, humidity, light, and pH) and critical stability attributes (such as polymorphism, particle size and surface area, water content, residual metals, and key excipients) that affect the stability of the drug substance and drug product (34).
Generally, the first lots of representative drug substance and drug product are put on stability per ICH conditions and time points. Although these representative lots may not be manufactured under cGMP, the stability data from these lots are often used in regulatory filings to support initial shelf-life and retest date assignments. Samples are placed on stability under at least two conditions, the long term storage condition (30 °C/65 or 75%RH or 25 °C/60%RH) to cover the intended use period and the accelerated condition (40 °C/75%RH) up to 6 months. Note that 30 °C/75%RH is required by certain countries in hot and humid climate zones. If 30 °C/65 or 75%RH is chosen as the long term condition, 25 °C/60%RH will be the backup long term condition, meaning that samples stored at 25 °C/60%RH are not analyzed unless stability under 30 °C/65 or 75%RH fails to meet specifications (31). For drug products with multiple strengths of the same formulation, a bracketing approach using the lowest and highest strengths to cover the entire range is acceptable and often used. The stability of drug substance can also be used to support the stability of simple, drug substance–based formulations such as PIC and powder in bottles (PIB).
The first GMP lot of drug substance and drug product can also be put on stability and tested at a reduced frequency, for example annually at the long term storage condition, to confirm the stability of an earlier representative lot. Not all GMP lots need to be placed on stability. When there are significant changes in the manufacturing process or manufacturing site, the conservative approach is to place one batch from the new process or site on stability. However, such an approach is not necessarily scientifically based without knowing whether the process or site changes likely affect the stability of the drug substance and drug product. Contrary to some common misconceptions, changes in manufacturing site and batch size per se without other changes have little stability impact; even changes in synthetic routes and impurity profiles do not necessarily make much difference. A more rational strategy based on scientific understanding of critical stability attributes and regulatory risk assessment has been advocated to enhance the value and efficiency of stability programs for early development, product registration, and post-approval stability (34).
Stability data are used to establish shelf-life or retest date and provide temperature excursion coverage. A two-year shelf-life is generally considered the minimum requirement for a viable commercial product. The initial retest date is typically based on extrapolation of stability data from accelerated conditions and should be confirmed by data from long term conditions. Extension of the initial retest date needs to be supported by additional long term stability data. The Arrhenius equation is commonly used to estimate the effect of temperature on the rate of chemical degradation. It does not apply to physical changes. For example, the rate of degradation at 40 °C is approximately five times faster than at 25 °C. Three months of stability at 40 °C can be used to project 12 months of stability at 25 °C. A word of caution in setting retest dates based on extrapolated stability is that some regulatory agencies do not accept retest dates more than 12 months beyond the available real time stability data from long term conditions (13).
Regulatory Filings
The importance of successful regulatory filings cannot be overstated. Pharmaceutical products cannot be marketed without the approval of the NDA or marketing authorization application (MAA), and clinical trials cannot start without clearance of the investigational new drug application (IND) or clinical trial application (CTA) by the health authority. Data generated by analytical chemists contribute to a large portion of the CMC sections of IND and CTA as well as NDA and MAA filings. Analytical chemists often are the authors of these sections.
The FDA has published a number of guidance documents for the preparation of INDs (35–38). There are some notable differences in INDs for US filings versus CTAs for non-US filings. For example, for phase 1 trials, INDs do not require the submission of detailed validation parameters or data, while the validation parameters and acceptance criteria are required for CTAs. A shelf-life or retest date is not required in the stability sections of the IND, while it needs to be explicitly stated in the CTA. Certain CMC sections often receive scrutiny from health authorities, such as specifications, control of genotoxic impurities, and shelf-life. Failure to satisfy regulatory inquires can result in a hold on clinical trials. The analytical chemist should work closely with the technical team and regulatory affairs to establish a well-defined control strategy, including well justified specifications and methods that are appropriate for the phase of development. Before any changes in specifications and methods are made, the impact on regulatory filings should be carefully assessed.
Summary and Conclusion
In this installment, the roles and responsibilities of the analytical chemist in quality control for small-molecule drug development have been discussed together with current practices and trends in setting specifications, method validation and transfer, release and stability testing, and regulatory filings. Many of the tests, techniques, and acceptance criteria used in QC are based on separation science, and applied in the context of drug development.
Acknowledgments
The authors would like to thank Jackson Pellett, Kelly Zhang, and Tania Ng of Genentech; Naijun Wu of Celgene; Raphael Ornaf of Vertex Pharmaceuticals; Beverly Nickerson of Pfizer; Anna Razynska of WES Pharma; Di Gao of AstraZeneca; and Szabolcs Fekete of University of Geneva for their input and editorial suggestions.
References
- Drug Discovery and Development: Technology in Transition, 2nd ed., R.G. Hill and H.P. Rang, Eds. (Churchill Livingston, Elsevier, Edinburgh, Scotland, 2012).
- R. Ng, Drugs: From Discovery to Approval (Wiley-Blackwell, Hoboken, New Jersey, 2009).
- D.K. Sarker, Quality Systems and Controls for Pharmaceuticals (Wiley, Hoboken, New Jersey, 2008).
- US Food and Drug Administration, “Pharmaceutical cGMP for the 21st Century--A Risk-Based Approach,” final report, (FDA, Rockville, Maryland, 2004).
- Code of Federal Regulations(CFR), Title 21, parts 210 and 211 (U.S. Government Publishing Office, Washington D.C.).
- US Food and Drug Administration, Guidance for Industry: Quality Systems Approach to Pharmaceutical CGMP Regulations (FDA, Rockville, MD, 2006).
- http://www.ich.org.
- US Food and Drug Administration, Guidance for Industry: cGMP for Phase 1 Investigational Drugs (FDA, Rockville, Maryland, 2008).
- https://iqconsortium.org.
- A. Eylath, T. Mazzeo, J.S. McElvain, B. Kleintop, A. Rignall, and J.W. Skoug, Pharm. Technol.36(6), 54–58 (2012).
- B. Kleintop, D. Chambers, G. Guo, H. Rasmussen, J. Spicuzza, K. Patterson, M. Szulc, S. Nowak, Z. Yuabova, S. Deegan, and K. Tombaugh, Pharm. Technol.36(7), 76–84 (2012).
- D. Joiner, E. Dokou, E. Schmitt, J. Skoug, M. Lovdahl, J. Creekmore, A. Eylath, and J. Pellett, Pharm. Technol. 36(8), 56–61 (2012).
- M. Alasandro, F. Diana, P. Curry, R. Timpano, S. Colgan, T. Mazzeo, J. Tan, B. Acken, Q.C. Li, and Z.J. Li, Pharm. Technol. 36(9), 64–70 (2012).
- D. O’Connor, J.S. McElvain, S. Zhang, K. Wong-Moon, M. Szulc, M. Yazdanian, F. Swanek, Z. Ge, M. Coutant, S.A. Miller, P. Yehl, and M.D. Trone, Pharm. Technol. 36(10), 86–94 (2012).
- International Conference on Harmonization, ICH Guideline Q6A, Specifications : Test Procedures and Acceptance Criteria for New Drug Substances and New Drug Products: Chemical Substances (ICH, Geneva, Switzerland, 1999).
- General Chapter <1112> “Application of Water Activity Determination to Nonsterile Pharmaceutical Products,” in United States Pharmacopeia 32-National Formulary 27 (United States Pharmacopeial Convention, Rockville, Maryland).
- US Food and Drug Administration, Guidance for Industry: Dissolution Testing and Specification Criteria for Immediate-Release Solid Oral Dosage Forms Containing Biopharmaceutics Classification System Class 1 and 3 Drugs (FDA, Rockville, Maryland, 2015).
- Genotoxic Impurities: Strategies for Identification and Control, A. Teasdale, Ed. (Wiley, Hoboken, New Jersey, 2011).
- C.J. Venkatramani and M.A. Al-Sayah, Amer. Pharm. Rev. 17(5), 64–70 (2014).
- International Conference on Harmonization, ICH Guideline M7, Assessment and Control of DNA Reactive (Mutagenic) Impurities in Pharmaceuticals to Limit Potential Carcinogenic Risk (ICH, Geneva, Switzerland, 2014).
- S.P. Boudreau, J.S. McElvain, L.D. Martin, T. Dowling, and S.M. Fields, Pharm. Technol. 28(11), 54–66 (2004).
- US Food and Drug Administration, Guidance for Industry, Analytical Procedures and Method Validation for Drugs and Biologics (FDA, Rockville, Maryland, 2015).
- HPLC for Pharmaceutical Scientists, Y.V. Kazakevich and R. LoBrutto, Eds. (Wiley, Hoboken, New Jersey, 2007), chapters 9 and 16.
- M.W. Dong, Modern HPLC for Practicing Scientists, (Wiley, Hoboken, New Jersey, 2006), chapter 7.
- H.T. Rasmussen, W. Li, D. Redlich, and M.I. Jimidar, in Handbook of Pharmaceutical Analysis by HPLC, S. Ahuja and M.W. Dong, Eds. (Elsevier/Academic Press, Amsterdam, the Netherlands, 2005), chapter 6.
- International Conference on Harmonization, ICH Guideline Q2 (R1) Validation of Analytical Procedures: Text and Methodology (ICH, Geneva, Switzerland, 2015).
- C. Choi and M.W. Dong, in Handbook of Pharmaceutical Analysis by HPLC, S. Ahuja and M.W. Dong, Eds. (Elsevier/Academic Press, Amsterdam, the Netherlands, 2005), chapter 6.
- E.J. Bishop, D. Kou, G. Manius, and H.P. Chokshi, in Sample Preparation of Pharmaceutical Dosage Forms, B. Nickerson, Ed. (Springer Science, New York, New York, 2011), chapter 10.
- I. Krull and M.E, Swartz, LCGC North Am. 24(11), 1204–1214 (2006).
- M.M. Nasr, Implementation of Quality by Design (QbD): Status, Challenges and Next Steps (Advisory Committee for Pharmaceutical Science, U. S. Food and Drug Administration, Rockville, Maryland, 2006).
- Handbook of Stability Testing in Pharmaceutical Development, K. Huynh-ba, Ed. (Springer, New York, New York, 2009).
- M.W. Dong, LCGC North Am. 33(10), 764–775 (2015).
- International Conference on Harmonization, ICH Guideline Q1B, Stability Testing: Photostability Testing of New Drug Substances and Products (ICH, Geneva, Switzerland, 1996).
- S.T. Colgan, T.J. Watson, R.D. Whipple, R. Nosal, J.V. Beaman, and D.M. De Antonis, J. Pharm. Innov. 7, 205–213 (2012).
- US Food and Drug Administration, Guidance on the Preparation of Investigational New Drug Products (Human and Animal), (FDA, Rockville, Maryland, 1991).
- US Food and Drug Administration, Guidance for Industry, Investigators, and Reviewers: Exploratory IND Studies (FDA, Rockville, Maryland, 2006).
- US Food and Drug Administration, Guidance for Industry: Content and Format of Investigational New Drug Applications (INDs) for Phase 1 Studies of Drugs, Including Well-Characterized, Therapeutic, Biotechnology-Derived Products (FDA, Rockville, Maryland, 1995).
- US Food and Drug Administration, Guidance for Industry: INDs for Phase 2 and Phase 3 Studies, Chemistry, Manufacturing, and Control Information (FDA, Rockville, Maryland, 2003).

Dawen Kou is a Scientist at Genentech, Small Molecule Analytical Chemistry and QC, responsible for multiple early-stage drug development projects. He was formerly a Senior Scientist at Roche, Nutley. He holds a PhD in Environmental and Analytical Chemistry from a joint program at Rutgers University and New Jersey Institute of Technology.

Larry Wigman is a Principal Scientific Manager at Genentech, Small Molecule Analytical Chemistry and QC. He was formerly an Associate Director at Sanofi and a senior manager at Mylan and Pfizer. He holds a PhD in Analytical Chemistry from Duke University.


Peter Yehl is a Director at Genentech, Small Molecule Analytical Chemistry and QC. He was formerly a Director at PTC Therapeutics and an Associate Director at Merck. He holds a PhD in Analytical Chemistry from University of Massachusetts at Amherst.

Michael W. Dong is a principal of MWD Consulting, focusing on training and consulting services in HPLC and UHPLC, pharmaceutical analysis and drug quality. He was formerly a Senior Scientist at Genentech, Small Molecule Analytical Chemistry and QC, Research Director at Synomics Pharma, Research Fellow at Purdue Pharma, and Senior Staff Scientist at Applied Biosystems / Perkin-Elmer. He holds a PhD in Analytical Chemistry from the City University of New York, and a certificate in Biotechnology from U. C. Santa Cruz. He has more than 100 publications including a best-selling book on chromatography. He is an editorial advisory board member of LCGC North America. Direct correspondence to: michael@mwd-consulting.com













 Headquarters complex in Washington, DC. | Image Credit: © Tada Images - stock.adobe.com")





